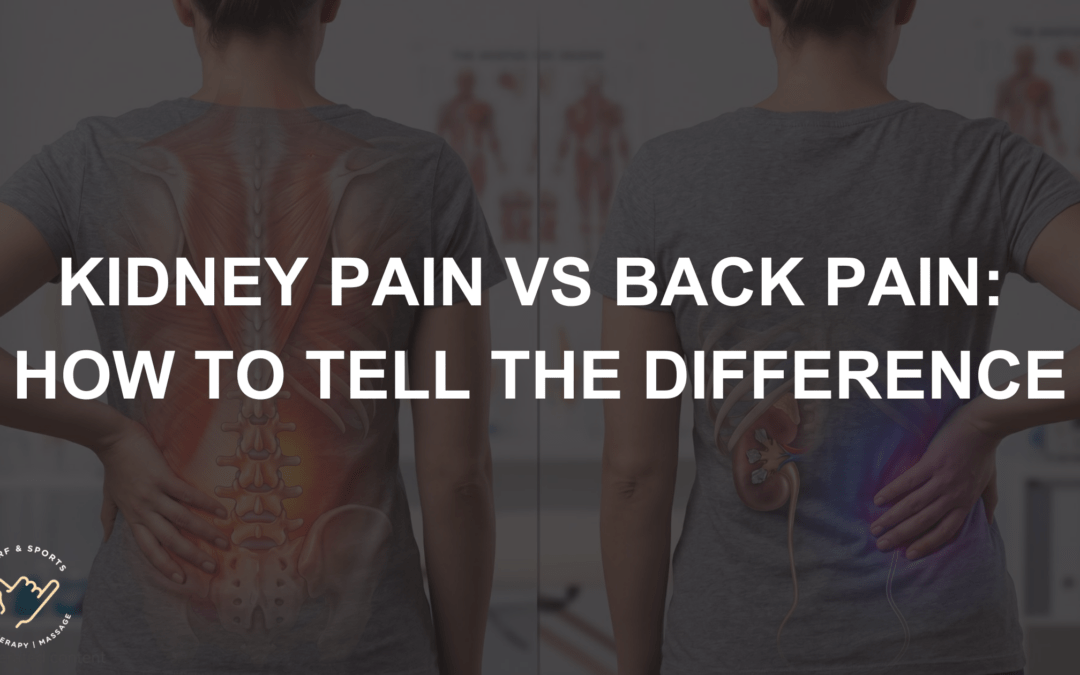
Kidney pain and back pain are two of the most commonly confused symptom presentations in adults. Both can produce a dull ache or sharp pain in the upper or lower back, both can worsen with certain positions, and neither clearly announces its cause.
The kidneys sit just below the rib cage on either side of the spine — close enough to the lumbar muscles and spinal structures that a problem in one system can feel indistinguishable from a problem in the other. Getting this distinction right matters: kidney-related pain requires medical assessment and often specific treatment, whereas mechanical back pain is the domain of soft-tissue and musculoskeletal care.
This article outlines the clinical differences between the two, the common causes of each, and the signs that point clearly toward one or the other.
Key Takeaways
- The kidneys sit beneath the rib cage on either side of the spine, which is why kidney pain is often felt in the same region as upper or lower back pain.
- Kidney pain tends to be deep, constant, and associated with urinary symptoms, fever, or flank tenderness — it does not typically change with movement or posture.
- Mechanical back pain is usually linked to activity, position, and movement — it worsens with sitting, standing, bending, or lifting, and eases with rest or certain positions
- Blood in the urine, fever, one-sided flank pain, and pain that radiates to the groin are red flags that warrant GP assessment, not soft tissue treatment
Where the Kidneys Actually Sit — and Why the Confusion Happens
The kidneys are two fist-sized organs that filter waste from the blood and produce urine. Each kidney sits in the posterior abdomen, nestled just below the rib cage on either side of the spine — roughly at the level of the lower thoracic and upper lumbar vertebrae. They are not located in the lower back, as many people assume, but higher up — tucked behind the abdominal organs and protected by the lower ribs.
This anatomy is the reason kidney pain is so frequently mistaken for back pain. The kidneys share the same regional space as the lumbar paraspinal muscles, the quadratus lumborum, and the lower thoracic spine. When one kidney becomes inflamed, infected, or obstructed, the pain it generates is felt in the same area — the flank, just below the rib cage on the affected side — where many people would naturally assume a muscle or spinal problem is located.
The confusion works the other way, too. Mechanical back pain originating from the lumbar spine, sacroiliac joint, or surrounding musculature can produce pain in exactly the region where kidney pain is felt. Without accompanying urinary symptoms or systemic signs, there is no obvious way for a patient to distinguish between the two based on the location of the pain alone.
What Kidney Pain Actually Feels Like
Kidney pain has several characteristics that help distinguish it from musculoskeletal back pain when they are present.
Location: Kidney pain is typically felt in the flank — the area between the lower ribs and the pelvis, on one or both sides of the back. It may radiate around to the front of the abdomen and downward toward the groin, depending on the cause.
Quality: The pain is often described as a deep, dull, constant ache. In the case of a kidney stone, the pain can become severe and colicky — arriving in intense waves as the stone moves through the ureter — and may radiate into the groin and inner thigh on the same side.
Response to movement: Kidney pain does not typically improve or worsen with changes in posture or spinal movement. Sitting, standing, walking, or lying down makes little consistent difference — unlike mechanical back pain, which almost always has a directional or positional component.
Associated symptoms: The presence of accompanying symptoms is the clearest indicator that pain has a renal rather than musculoskeletal origin. These include:
- Changes in urination — increased frequency, pain or burning when urinating, difficulty urinating, or reduced output
- Blood in the urine (haematuria) — which may make urine appear pink, red, or brown
- Fever or chills — indicating a kidney infection (pyelonephritis) requiring antibiotic treatment
- Nausea or vomiting
- Oedema — swelling in the legs or ankles, which can indicate impaired kidney function
A kidney infection can cause significant back and flank pain alongside systemic symptoms, including fever, fatigue, and urinary changes. Kidney disease more broadly is often described as a silent condition — many people lose substantial kidney function before any symptoms appear, which is why back pain accompanied by urinary changes or unexplained fatigue warrants investigation rather than assumption.
What Mechanical Back Pain Feels Like
Mechanical back pain — the most common type of back pain — originates from the muscles, ligaments, intervertebral discs, facet joints, or sacroiliac joint of the lumbar and thoracic spine. It accounts for the vast majority of back pain presentations in otherwise healthy adults.
Location: Mechanical back pain is most commonly felt in the lower back, though it can occur anywhere along the spine. It may radiate into the buttock or down the leg if a nerve is compressed — a pattern known as sciatica, typically associated with disc herniation or lumbar nerve root irritation.
Quality: The pain varies from a dull, persistent ache to sharp or stabbing pain with specific movements. Stiffness — particularly in the morning or after prolonged sitting — is a common feature.
Response to movement: the key distinguishing characteristic. Mechanical back pain is almost always positional or movement-dependent. It typically worsens with prolonged sitting or standing, bending forward, lifting, or certain spinal movements — and eases with rest, a change of position, or gentle movement. This directional or activity-related quality is rarely present in kidney pain.
Associated symptoms: Mechanical back pain does not produce urinary symptoms, fever, or systemic signs unless a separate condition is also present. Nerve compression from a disc or sacroiliac joint dysfunction may cause numbness, tingling, or weakness in the leg, but these are musculoskeletal rather than urological in origin.
Kidney Pain vs Back Pain: A Clinical Comparison
Kidney Pain | Mechanical Back Pain | |
Location | Flank — below the rib cage, one or both sides | Lower back may radiate to the buttocks or leg |
Quality | Deep, constant, dull ache; colicky waves with kidney stones | Dull ache, sharp with movement, stiffness |
Response to movement | Unchanged by posture or spinal movement | Worsens with specific movements, postures, or activity |
Associated symptoms | Urinary changes, fever, nausea, haematuria, oedema | Leg pain, numbness, tingling from nerve compression |
Onset | Often sudden or progressive with no clear physical trigger | Usually follows a physical activity, awkward movement, or prolonged posture |
Touch sensitivity | Tender to firm pressure over the kidney area (costovertebral angle tenderness) | Tenderness over the lumbar muscles, SI joint, or spinal structures |
Who to see | GP — requires urinalysis, imaging, and possible antibiotics or intervention | Myotherapist, physiotherapist, or GP, depending on severity |
Common Causes of Kidney Pain
Understanding the underlying conditions that produce kidney pain helps clarify when a GP assessment is necessary:
Kidney infection (pyelonephritis): A bacterial infection of one or both kidneys, typically ascending from a urinary tract infection. Produces flank pain, fever, and urinary symptoms. Requires antibiotic treatment.
Kidney stones: Solid mineral deposits that form in the kidneys and may pass through the ureter. Kidney stone pain is often described as severe, colicky, and radiating toward the groin. Small stones may pass without intervention; larger stones may require medical management.
Urinary tract infection (UTI): While primarily affecting the bladder, an untreated UTI can spread to the kidneys. Lower back discomfort, burning urination, and urinary frequency are common features.
Kidney cysts: Fluid-filled sacs on one or both kidneys, which are often asymptomatic but can cause flank pain when large or in the context of polycystic kidney disease.
Kidney cancer: A less common but serious cause of kidney pain, typically presenting with flank pain, haematuria, and unexplained weight loss. Medical investigation is essential.
Chronic kidney disease often produces no pain until it is significantly advanced. When pain is present, it may be felt in the back below the ribs. Swelling, fatigue, and changes in urine output are more common early indicators.
Common Causes of Mechanical Back Pain
For comparison, the most frequent causes of mechanical back pain include:
- Muscle strain or ligament sprain — often from heavy lifting, awkward movement, or accumulated postural load
- Intervertebral disc herniation — where disc material protrudes and presses on a spinal nerve, potentially causing sciatica
- Sacroiliac joint dysfunction — pain at the junction between the sacrum and pelvis, often one-sided and activity-related
- Facet joint irritation — producing localised spinal pain with rotation or extension
- Poor posture and muscular imbalance — accumulated through prolonged sitting, sedentary work, or repetitive physical demands
- Myofascial trigger points — active trigger points in the lumbar paraspinals or quadratus lumborum that refer pain across the lower back
Red Flags: When Back Pain Needs Urgent Medical Assessment
Some presentations require immediate medical attention regardless of whether the pain feels muscular or renal in origin. See a GP or seek urgent care if back pain is accompanied by:
- Blood in the urine — always requires investigation
- Fever or chills alongside back pain — may indicate a kidney infection or other systemic cause
- Pain that radiates to the groin — a characteristic pattern of kidney stone movement through the ureter
- Severe, sudden-onset flank pain — particularly one-sided, which may indicate kidney stone obstruction or a vascular event
- Unexplained weight loss with back pain warrants investigation to exclude a neoplasm or kidney cancer.
- Loss of bladder or bowel control alongside back pain — a potential sign of cauda equina syndrome, which is a medical emergency
- Back pain following significant trauma — such as a fall, road accident, or direct impact
- Back pain that is constant, severe, and completely unaffected by rest or movement — particularly in adults over 50 or those with a history of cancer
None of these presentations is appropriate for self-treatment or initial soft tissue management. A GP assessment — including urinalysis, blood tests, and imaging where indicated — is the right first step.
When Myotherapy Is and Is Not Appropriate
Myotherapy is appropriate for confirmed mechanical back pain — including muscle strain, trigger-point referral, sacroiliac joint dysfunction, disc-related sciatica, and postural or biomechanical contributors to lumbar pain. The myotherapy team at Surf & Sports Myotherapy works through the soft-tissue and movement contributors to back pain, directly addressing the cause rather than just the symptom location.
Myotherapy is not appropriate as a first response to back pain that has urinary symptoms, fever, or any of the red flags listed above. If investigations confirm that the kidneys are the source of pain, soft tissue treatment to the back will not address it, and may delay appropriate care.
If you have already had a medical assessment and the kidneys have been ruled out as a contributing factor. Still, your back pain persists, a myotherapy assessment can identify what is driving the mechanical component of your presentation.
From the Clinic, “The question ‘is this my kidneys or my back?’ comes up more than most people might expect — particularly with one-sided upper lumbar pain. The pattern of the pain, whether urinary symptoms are present, and how the pain responds to movement are the three things that help clarify this clinically. When someone describes severe pain that builds and eases in waves and has travelled toward the groin, that is a GP conversation — not a treatment session. When the pain is activity-related, directional, and eases with rest, it is almost certainly mechanical.”
For the broader clinical context of how visceral organs produce pain that appears to come from the spine or surrounding musculature, the clinic’s guide on referred pain and symptom confusion covers the neurological basis in detail.
Frequently Asked Questions
Can a kidney infection cause lower back pain without urinary symptoms?
In some cases, yes — particularly in older adults or people with compromised immune function, urinary symptoms may be absent or subtle even when a kidney infection is present. If back pain is accompanied by fever, fatigue, or general unwellness without an obvious physical trigger, a GP assessment including urinalysis is worthwhile to exclude a renal cause.
How do I tell if my back pain is muscular or from the kidneys?
The most reliable indicator is how the pain responds to movement and posture. Muscular back pain almost always changes with activity — worsening with sitting, bending, or lifting, and easing with rest or gentle movement. Kidney pain tends to be constant and unaffected by spinal movement. The presence of urinary symptoms, fever, or flank tenderness also points strongly toward a renal cause.
Can you have kidney pain and back pain at the same time?
Yes. A kidney infection or stone can cause renal flank pain at the same time as an unrelated mechanical back pain is present. In these cases, the two presentations may be difficult to separate without a clinical assessment. If any urinary symptoms or systemic signs are present alongside back pain, a GP should assess both possibilities.
Will a remedial massage help kidney pain?
No. Remedial massage addresses soft tissue and musculoskeletal dysfunction — it does not treat the kidney itself or the conditions that cause kidney pain. If kidney pain is the source, soft tissue treatment will not provide meaningful relief and should not be used as a substitute for appropriate medical care.
When is it safe to see a myotherapist for back pain without seeing a GP first?
If back pain followed a clear physical trigger — lifting, a sudden awkward movement, or accumulated postural load — and is not accompanied by urinary symptoms, fever, unexplained weight loss, leg weakness, or bladder and bowel changes, a myotherapy assessment is a reasonable first step. If any of those features are present, a GP assessment should come first.
The Right Care Starts With the Right Assessment
Back pain is common. Kidney-related pain presenting in the back is less common but easy to miss without knowing what to look for. The distinction matters because the treatment pathways are entirely different — and mistaking one for the other can delay care that genuinely needs to happen.
If your back pain fits the mechanical pattern — activity-related, positional, without systemic symptoms — the team at Surf & Sports Myotherapy in Noosaville can assess and treat the musculoskeletal contributors directly.
If there is any uncertainty, or if urinary symptoms, fever, or any of the red flags above are present, a GP is the right starting point.
Book your appointment online or call 0423 729 694.
Opening hours: Monday–Friday 08:00–19:00 | Saturday 08:00–16:00 Location: 3/14 Thomas St, Noosaville QLD 4566

About the Author
Gary Javonena is the founder of Surf & Sports Myotherapy and holds an Advanced Diploma of Myotherapy from RMIT University.
Gary’s clinical work includes the assessment of complex musculoskeletal presentations in which referred pain, postural dysfunction, and systemic contributors intersect — including cases in which gastrointestinal function directly contributes to lumbar pain patterns. Meet the full team.
Related posts
Alcohol and Muscle Recovery: What Happens to Your Body the Day After Drinking
Most people are aware that drinking heavily the night before training is not ideal. What is less...
Dehydration and Muscle Soreness: How Much Water Actually Matters for Recovery
The relationship between hydration and muscle soreness is more specific than the general advice to...
Vitamin D Deficiency and Chronic Muscle Aches – A Hidden Cause
Queensland is one of the sunniest places on Earth, and the Sunshine Coast lives up to its name —...